COMPARISON OF THE THERAPEUTIC EFFICACY OF PHONOPHORESIS AND CRYOTHERAPY AS COMBINED THERAPY IN THE MANAGEMENT OF REPETITIVE STRAIN INJURY (RSI) : Vinod Nair *
OBJECTIVES
Repetitive strain injuryis the single largest category of workplace injuries and is responsible for almost 30% of all workers in companies.Repetitive strain injury (RSI) is a general term used to describe the pain felt in muscles, nerves and tendons caused by repetitive movement and overuse. This study was designed to compare the therapeutic efficacy of Phonophoresis and cryotherapy as combined therapy in the management of repetitive strain injury(RSI).
METHODS
Sixty (60) subjects were assigned randomly to one of three groups: Double-modality therapy (DMT) group (n=20) received cryotherapy and 15% methyl salicylate phonophoresis, PHONOPHORESIS group (n=20) received 15% methyl salicylate phonophoresis and CRYOTHERAPY group (n=20) received cryotherapy.
Ultrasound at an intensity of 2 W/cm² and frequency of 1MHz was used to apply methyl salicylate while intermittent cryotherapy was the mode of application. Subjects? pre- and post-treatment pain perception scores (PPS) using visual analogue scale (VAS) were assessed and the sessions of treatment in all groups were recorded. Treatment was administered on alternate days and discharges were made in all groups when subjects were pain free.
RESULTS
The study has demonstrated therapeutic efficacy of DMT, but it was not superior to the single treatment protocol of phonophoresis or cryotherapy. However, it might take fewer sessions in the DMT group to treat and make more than 90% of the patient’s pain free and fit to return to active performance.
KEYWORDS : Cryotherapy, Double-modality therapy, Repetitivestraininjury, Phonophoresis, Ultrasound
OBJECTIVES
Repetitive strain injury is the single largest category of workplace injuries and is responsible for almost 30% of all workers in companies. Repetitive strain injury (RSI) is a general term used to describe the pain felt in muscles, nerves and tendons caused by repetitive movement and overuse. This study was designed to compare the therapeutic efficacy of Phonophoresis and cryotherapy as combined therapy in the management of repetitive strain injury (RSI).
METHODS
Sixty (60) subjects were assigned randomly to one of three groups:
Double-modality therapy (DMT) group (n=20) received cryotherapy and 15% methyl salicylate phonophoresis, PHONOPHORESIS group (n=20) received 15% methyl salicylate phonophoresis and CRYOTHERAPYgroup (n=20) received cryotherapy.
Ultrasound at an intensity of 2 W/cm² and frequency of 1MHz was used to apply methyl salicylate while intermittent cryotherapy was the mode of application. Subjects? pre- and post-treatment pain perception scores (PPS) using visual analogue scale (VAS) were assessed and the sessions of treatment in all groups were recorded. Treatment was administered on alternate days and discharges were made in all groups when subjects were pain free.
RESULTS
The study has demonstrated therapeutic efficacy of DMT, but it was not superior to the single treatment protocol of phonophoresis or cryotherapy. However, it might take fewer sessions in the DMT group to treat and make more than 90% of the patient’s pain free and fit to return to active performance.
KEYWORDS: Cryotherapy, Double-modality therapy, Repetitive strain injury, Phonophoresis, Ultrasound
INTRODUCTION
Repetitive strain injury (RSI) which are usually due to strenuous activity account for roughly 30% of patient complaints in the primary health care settings (Childs et al, 2005) and are a leading cause of work absenteeism worldwide (Beeb et al, 2005). Repetitive strain injury constitutes the largest proportion of injuries among athletes (Reilly and Hardiker, 1983). Report has indicated that more than 60% of men and women who work on the computer have complained of pain resulting from various RSI (Idowu et al, 2005). The most common term used to describe these disorders is musculoskeletal injury (MSI). Some examples of repetitive strain injury are Carpal Tunnel Syndrome, Tendinitis, Tenosynovitis and Bursitis. Common symptoms are Pain in the hands, arms, shoulders, neck, back, legs or feet and May include swelling, numbness, tingling and a feeling of heaviness and/or tiredness in the affected area Some workers may experience multiple symptoms due to more than one injury Low back pain (LBP) is not only one of the most common musculoskeletal injury in industrialised societies, but it is the most costly, and it is the primary cause of disability in persons under age 45 years (DeRosa and Porterfield,1992).
Physical treatments (i.e phonophoresis, cryotherapy, etc.) have been used for many years and are currently being used to reduce pain, control swelling or inflammation and improve or restore function in the management of RSIs. Phonophoresis which is the use of ultrasound (US) to enhance percutaneous absorption of topical drugs in the management of RSIs and dermatological conditions has been a widely applied clinical therapeutic procedure. It is believed to accelerate functional recovery by decreasing pain and promoting healing. In a comparative study involving iodex phonophoresis (n = 15), iodex iontophoresis (n = 15) and a placebo (n = 15) in the management of shoulder periarthritis, Bumin and Can (2004) did observe that iodex phonophoresis and iodex iontophoresis were significantly effective in decreasing pain as compared to the placebo. The application of cold (otherwise known as cryotherapy) for the treatment of injury or disease, particularly for increasing pain threshold, decreasing inflammatory reaction and spasm following MSIs (Swenson et al, 1996; Yagiz, 2006) has been advocated by some researchers as the sole treatment to be used during all phases of soft tissue injury (Cote et al, 1988; Swenson et al, 1996). In a systematic review of some randomised controlled trials (RCTs) to indentify the efficacy of ice in the management of pain and swelling resulting from soft tissue injury, it is reported that cryotherapy seems to be effective in decreasing pain and speeds return to full activity (MacAuley, 2001; Hubbard and Denagar, 2004). Phonophoresis or Cryotherapy in isolation or in combination with other therapies has become widely used regimen for reducing pain, inflammation and improving or restoring function in managing RSIs (Kellett, 1986; Palmer and Toombs, 2004; Wilson and Best, 2005). Davis (1991) has recommended the application of cryotherapy as a single treatment protocol for hours (i.e 72 hours) when there is trauma (i.e rotator cuff syndrome) before resorting to phonophoresis for the remaining period of treatment. Literature has indicated that cold application prior to phonophoresis produces an intense hyperemia which may improve the absorption and distribution of the medication to effect pain relief and resolution of inflammation (Santiesteban, 1983). The recognition of the importance of pain control in the recovery from RSIs to enable the injured persons return to participation (athletes) or return to work (typical population) has prompted clinicians to continue to explore more aggressive pain management strategies (Brolinson and Sampson, 2003; Hubbard et al, 2004). Some reports (Santiesteban, 1983; Balogun, 1990) suggested that phonophoresis and cryotherapy can be combined (double-modality therapy – DMT) in the management of RSIs for better outcome. Sequel to this, pain clinics and sport centres have adopted as a tradition the treatment protocol of combining phonophoresis and cryotherapy (DMT) in the management of RSIs worldwide. Despite the general acceptance and the frequency at which this treatment approach (DMT) is being practiced, there is dearth in the literature to support the practice or demonstrate its efficacy or superiority over the single treatment protocol (Balogun, 1990; Ball, 2002). The practice is probably or largely based on anecdotal evidence rather than on empirical data. Clinical opinion just isn’t good enough anymore. Hence, it is incumbent upon the clinician or the therapist to collect information or data to support clinical decision making with something more than physiologic philosophy based on opinion. Randomised clinical trials are required therefore, to support clinical decision making on the use of phonophoresis and cryotherapy as combined treatment (DMT) protocol for optimal outcome or response following RSI management.
MATERIALS AND METHODS
Sixty (60) patients (40 males, 20 females; mean 34 years; range 18 to 70 years) who sustained repetitive strain injury were all recruited as they presented before the physician for treatment at the various hospitals in Udaipur. Only subjects who sustained not more than one repetitive strain injury (i.e subjects with multiple injuries were not eligible) with acute onset of symptoms or occurring as an acute exacerbation of chronic lesion were included in the study. Subjects who were on any form of analgesics (steroids and non-steroidal antiinflammatory drugs – NSAIDs), muscle relaxants and any form of physiotherapy treatments were all excluded from the study. Subjects with open wounds over the injury sites, pregnancy, disease conditions (e.g thrombophlebitis, cardiac disease patient with pacemaker, tumour, etc) and those allergic to topical methyl salicylate or cold which contra-indicate the treatment protocols used in this study were all excluded. The use of NSAIDs or analgesics and any other form of treatment was not permitted or allowed throughout the study period. Before entry into the study all subjects voluntarily signed the informed consent forms after the protocol for the trial was explained to them. All procedures involving the subjects met criteria.
PROCEDURE
On completion of history, careful clinical and radiographic examination the sixty (60) subjects whose injuries were classified as follows :- rotator cuff syndrome (n=10), ankle sprain (n=8), knee sprain (n=6), patellar bursitis (n=7), low back pain (n=12), muscle strain (n=11), tennis elbow (n=3), hamstring tendinitis (n=2), De Quervain tenosynovitis (n = 1) were randomly assigned to one of three treatment groups:
(i) Double-modality Therapy (phonophoresis and cryotherapy combined) (n = 20)
(ii) Phonophoresis Group (n = 20)
(iii) Cryotherapy Group (n = 20)
An independent researcher generated the randomisation sequence by writing the treatment groups and placed in sequentially numbered opaque sealed envelopes which were used to assign the subjects to their respective groups. Neither the primary researchers nor any other person that was involved in treatment allocation were aware of the randomisation schedules (Brolinson and Sampson, 2003). The ultrasound machine and the transducer ( 1MHz and 3MHz treatment head) were all tested and certified functional. Subjects pain perception was subjectively assessed or measured and recorded using a 10cm visual analogue scale (VAS) marked “no pain” at one end and “worst pain ever” at the other end. After the subjects were carefully educated on the use of VAS and it was observed that subjects could identify their pain levels or scores on the scale without any difficulties. This form of assessment was considered most appropriate because of its high level of repeatability when used serially on the same patient. Sensory test was conducted among the subjects to ascertain that there was no sensory loss. Subjects were instructed and made to understand that at no time during phonophoresis should they suffer discomfort. There might be a sensation of very mild warmth, but other than that only the pressure and the movement of the transducer should be felt. Any other sensation should be reported at once. All subjects assigned to cryotherapy were made to understand that sensation like cold, burning, aching and numb (Kellett, 1986) would be felt during the treatment procedure which causes no harm. Finally, subjects were comfortably supported and positioned to maximise circulation to the area being treated when they were ready for treatment.
The subjects in DMT group (n = 20) received cryotherapy and phonophoresis as combined therapy (DMT). Intermittent cryotherapy (MacAuley, 2001; Bleakley et al, 2006) using ice pack (16cm x 12cm) was applied directly over the patients conditions for 10 minutes. The ice pack was then removed after the initial 10 minutes application and allowed the treatment part to rest at room temperature for 10 minutes. The ice pack was reapplied immediately following the expiration of the rest period for another 10 minutes (total cryotherapy period = 20 minutes). At the expiration of the second ice pack application the treatment part was cleansed with a towel and continuous ultrasound at an intensity of 2 W/cm² and frequency of 1MHz was used to apply 1.5g of 15% methyl salicylate cream thoroughly mixed with 1.5g of aquasonic gel as coupling medium for 6 minutes. The ultrasound head was moved over the part under treatment about one-half (1½) the width of the transducer at approximately 2 to 4 cm/sec; using small, continuous and overlapping circular movements to avoid or prevent periosteal pain (Santiesteban, 1983). These treatment values or settings were selected to capture both the thermal and non thermal effects of ultrasound in other to optimize transdermal methyl salicylate 15% delivery (Byl, 1995; Cagnie et al, 2003). The subjects in PHONO group (n = 20) received a “live” phonophoresis as a single treatment protocol. The treatment procedure (phonophoresis) was exactly the same as applied in DMT group. All subjects in CRYO group (n = 20) received cryotherapy. Intermittent cryotherapy was applied directly over the subjects? conditions with the same procedure described in DMT group. At the expiration of cryotherapy application, the treatment part was cleansed with a towel Treatments were administered on alternate days in each group until subjects were fit for discharge. At the end of weeks 1, 2, 3 and 4 after treatment in each group, subjects posttreatment pain perception scores (PPS) were assessed and recorded.
Assssment and recording of pre-and post-treatment pain perception scores (PPS) were blinded from the researchers to reduce or eliminate bias (assessment by neutral assessors). Treatments were terminated and subjects discharged in all groups when subjects felt pain was sufficiently relieved and no longer needed treatment.
STATISTICALANALYSIS
Descriptive and inferential statistics using the Statistical Packages for the Social Sciences (SPSS) was used for data analysis. Independent and paired mean difference tests (t – test) were used to compute subjects repeated measures within all groups while a one – way ANOVA (Klaiman et al, 1998) was used to compute measures across the groups with the level of significance for all tests set at 0.05.
RESULTS
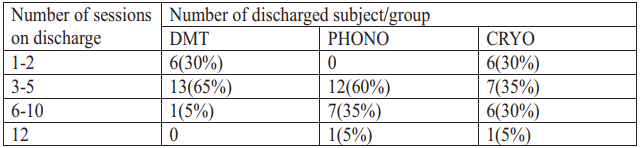
Two hundred and seventy-five (275) treatment sessions were recorded in all the groups – 72 (26.2%) was recorded in the DMT group, 105 (38.2%) recorded in the PHONO group while the CRYO group recorded 98 (35.6%) respectively. The result indicates no statistical significant (P>0.05) difference in the mean treatment sessions between the three groups. The number of subjects discharged on or before completion of treatment term in all the three groups is presented in Table 1. While all subjects were fit for discharge without necessarily completing the 12 sessions of treatment (initially designed for the study) in DMT group, 5% (1) of the subjects in CRYO and PHONO groups received the full term treatment (i.e. 12 sessions of treatment) respectively. Nineteen ( 95%) subjects in the DMT group were fit for discharge after receiving treatment for 1 to 5 sessions. Only 12 (60%) and 13 (65%) subjects in PHONO and CRYO groups respectively were fit for discharge after the same duration of treatment. While no subjects were fit for discharge in the PHONO group after receiving 1 to 2 treatment sessions, the DMT and CRYO groups recorded 6 (30%) discharges respectively. Furthermore, at the completion of 10 sessions of treatment, DMT group had discharged all subjects (100%) pain free while PHONO and CRYO group recorded 95% discharges respectively.
Table 1: Subject Discharge Pattern
 DMT=Double-Modality Therapy (Phonophoresis + Cryotherapy), PHONO = Phonophoresis, CRYO = Cryotherapy
DMT=Double-Modality Therapy (Phonophoresis + Cryotherapy), PHONO = Phonophoresis, CRYO = Cryotherapy
Table 2. Comparison of pain Perception Scores
 DMT=Double-Modality Therapy (Phonophoresis + Cryotherapy), PHONO = Phonophoresis, CRYO = Cryotherapy *=P<0.05
DMT=Double-Modality Therapy (Phonophoresis + Cryotherapy), PHONO = Phonophoresis, CRYO = Cryotherapy *=P<0.05
Table 2 shows that the three modalities (DMT, PHONO and CRYO) were equally and significantly (P< 0.05) effective in producing optimal pain relief among the subjects and no group was superior to the other. No subject complained of any discomfort or adverse effect; such as periosteal pain, skin allergy, frostbite or nerve palsy; instead the subjects reported treatments were effective, tolerable and pleasant. All subjects felt satisfied with their level of pain relief and requested for discharge accordingly.
DISCUSSION
The use of phonophoresis and cryotherapy in isolation or in combination with other therapies in the management of repetitive strain injury has been widely reported. They are widely used regimen for reducing pain, inflammation and improving function. On the contrary, the use of phonophoresis and cryotherapy as combine therapy (DMT) protocol has gained general acceptance and popularity in the clinical setting, but there is no existing clinical trial in the literature to suggest or indicate its efficacy (Ball, 2002). This study is the first that has reported with empirical data the efficacy of DMT. The study has further indicated that DMT was not superior to the single treatment protocol of phonophoresis or cryotherapy which has debunked the belief that has been probably or largely based on anecdotal evidence (Santiesteban, 1983; Balogun, 1990).
The groups did not show significant difference in the overall discharge pattern. The DMTgroup discharged all subjects (100%) after 10 sessions of treatment while PHONO and CRYO group discharged 95% of their subjects who were pain free. However, the discharge pattern in the DMT group suggests it might take fewer sessions (about 5 sessions) to treat and make more than 90% of the subjects with the type of repetitive strain injury (RSI) included in this study pain free, side effect free and fit to return to active performance. The fewer treatment sessions may be an advantage for the subjects (patients), the employer and the clinician. On the part of the subjects, absenteeism from work to keep hospital treatment appointments and subsequent loss of work hours is minimized; while the workload usually experienced by the clinician may be reduced. On the other hand, with the pressure to treat athletes who sustained RSI safely and efficiently in order to get them back to effective performance as quickly as possible (Hubbard et al, 2004), DMT protocol may have an edge or advantage over other modalities.
Phonophoresis and cryotherapy have demonstrated significant pain relief among the subjects in this study which has corroborated the works of Klaiman et al (1998), Kozanoglu et al (2003), and Hubbard and Denegar (2004). This has further reduced the inconsistency or controversies associated with the level of efficacy of the modalities. Phonophoresis simply produces thermal effect from the ultrasound which increases kinetic energy of molecules in the drug and in the cell membrane, dilates points of entry such as hair follicles and the sweat glands, and increases the circulation to the treated area (Byl, 1995; Cagnie et al, 2003). These physiological changes enhance the opportunity for drug molecules (e.g methyl salicylate 15%) to diffuse through the stratum corneum (SC) and be collected by the capillary network in the dermis (Byl, 1995), thereby initiating pain relief. The mechanism by which cryotherapy decreases pain after injury is however a contentious issue (Bleakly et al, 2006). Pain relief with cold application could be due to altered nerve conduction velocity (NCV), inhibition of nociceptors, etc. (Algafly and George, 2007; Herrera et al, 2010). Intermittent cryotherapy application helps sustain reduced muscle temperature without compromising the skin and allows the superficial skin temperature to return to normal while the deeper muscle temperature remains low (MacAuley, 2001).
The current study has indicated significant therapeutic efficacy of DMT, but it was not superior to the single treatment protocol of phonophoresis or cryotherapy. However, the discharge pattern in the DMT group suggests it might take fewer sessions (about 5 sessions) to treat and make more than 90% of the subjects with the type of repetitive strain injury (RSI) included in this study pain free, side effect free and fit to return to active performance.
REFERENCES
1. Cleland LG. “RSI”: a model of social iatrogenesis. Med J Aust. 1987 Sep 7;147(5):236-239. [PubMed]
2. Harrington JM, Carter JT, Birrell L, Gompertz D. Surveillance case definitions for work related upper limb pain syndromes. Occup Environ Med. 1998 Apr;55(4):264-271. [PMC free article] [PubMed]
3. Helliwell PS. Diagnostic criteria for work-related upper limb disorders. Br J Rheumatol. 1996 Dec;35(12):1195-1196. [PubMed]
4. McNaughton H. The label ‘Occupational Overuse Syndrome’: time to change. N Z Med J. 2000 May 26;113(1110):193-194. [PubMed]
5. Mackinnon SE, Novak CB. Repetitive strain in the workplace. J Hand Surg Am. 1997 Jan;22(1):2- 18.[PubMed]
6. Wigley RD. Repetitive strain syndrome–fact not fiction. N Z Med J. 1990 Feb 28;103(884):75- 76.[PubMed]
7. Allen L.V.(2005). Compounding for Phonophoresis. Secundum Artem. 11(2) : 1-6.
8. Ball A.M.(2002). Phonophoresis and Ice (PTupdate) URL=http://www.PTupdate.com. Accessed on 2/9/11 & 4/4/12.
9. Balogun J.A. (1990). Recent Advances in Electrotherapy. Journal of Nigeria Association of Sports Science and Medicine. 1: 1-12.
10. Beebe F.A., Barkin R.L. and Barkin S. (2005). A Clinical and Pharmacological Review of Skeletal Muscle Relaxants for Musculoskeletal Conditions. American Journal of Therapeutics. 12 (2) : 151 – 171.
11. Bleakley C.M., McDonough S.M., MacAuley D.C. and Bjordal J. (2006). Crytherapy for Acute Ankle Sprains – A Randomised Controlled Study of Two Different Icing Protocols. British Journal of Sports Medicine. 40 (8) : 700 – 705.
12. Bolin D.J. (2003). Transdermal approaches to pain in soft tissue injury. Curr. Sports Med. Rep. 2 (6):303 – 309.
13. Brolinson P.G. and Sampson M. (2003). Pathophysiology of pain in sports. Curr. Sports Med. Rep. 2 (6):310 – 314 (Abstract).
14. Bumin G. and Can F. (2004). Effects of iontophoresis and phonophoresis methods on pain cases with shoulder periarthritis. Pain Clinic. 13 (2): 159 – 162 (Abstract online).
15. Byl N.N. (1995). The use of Ultrasound as an enhancer for Transcutaneous Drug Delivery: Phonophoresis. Physical Therapy. 75 (6) : 539 – 553.
16. Cagnie B., Vinck E., Rimbaut, S. and Vanderstraeten G. (2003). Phonophoresis Versus Topical Application of Ketoprofen: Comparison Between Tissue and Plasma Levels. Physical Therapy. 83 (8) : 707 – 712.
17. Childs J.D., Whitman J.M., Sizer P.S., Pugia M.L., Flynn T.W. and Delitto A.(2005). A description of physical therapists? knowledge in managing musculoskeletal conditions. BMC Musculoskeletal Disorders. 2005, 6:32 : 1471 – 1483.
18. Ciccone C.D., Leggin B.G. and Callamaro J.J. (1991). Effects of ultrasound and trolamine salicylate phonophoresis on delayed – onset muscle soreness. Physical Therapy. 71 (9): 666 – 675.
19. Cote D.J., Prentice W.E., Hooker D.N. and Shields E.W. (1988). Comparison of Three Treatment Procedures for Minimizing Ankle Sprain Swelling. Physical Therapy. 68 (7) : 1072 – 1076.
20. Davis R.V. (1991). Management of Rotator Cuff Syndrome. Dynamic Chiropractic. 9 (9) : 26 – 28.
21. DeRosa C.P. and Porterfield J.A.(1992). A Physical Therapy Model for the Treatment of Low Back Pain. Physical Therapy. 72 (4) : 261 – 272.
22. Hootman J.M., Macera C.A., Ainsworth B.E., Anddy C.L, Martin M. and Blair S.N. (2002). Epidemiology of Musculoskeletal injuries among sedentary and physically active adults. Medicine and Science in Sports and Exercise. 34 (5) : 838 – 844
23. Hoppenrath T. and Ciccone C.D.(2006). Is there evidence that phonophoresis is more effectivethan ultrasound in treating pain associated with lateral epicondylitis? Physical Therapy. 86 (1)
24. Hubbard T.J. and Denegar C.R. (2004). Does Crytherapy Improve Outcomes With Soft Tissue Injury? Journal of Athletic Training. 39 (3) : 278 – 279.
25. Idowu P.A., Adedoyin R.A. and Adagunodo R.E. (2005). Computer Related Repetitive Strain Injuries. Journal of Nigeria Society of Physiotherapy. 15 (1):13 – 18
26. Kellett J. (1986). Acute soft tissue injuries – a review of the literature. Medicine and Science in Sports and Exercise. 18 (5) : 489 – 499.
27. Klaiman M.D., Shrader, J.A., Danoff J.V., Hicks J.E., Pesce W.J. and Ferland J. (1998). Phonophoresis versus ultrasound in the treatment of common musculoskeletal conditions. Medicine and Science in Sports and Exercise. 30 (9):1349- 1355(Abstract)
28. Kozanoglu E., Basaran S., Guzel R. and Guler-Uysal F. (2003). Short term efficacy of ibuprofen phonophoresis versus continuous ultrasound therapy in knee osteoarthritis. Swiss Medical Weekly. 133 : 333 – 338.
29. Kuntz A.R., Griffiths C.M., Rankin J.M., Amstrong C.W. and McLaughlin, T.J. (2006). Cortisol Concentrations in Human Skeletal Muscle Tissue After Phonophoresis with 10% Hydrocortisone Gel. Journal of Athletic Training. 41 (3):321 – 324.
30. MacAuley D.C. (2001). Ice Therapy – how good is the evidence? International Journal of Sports Medicine. 22(5):379 – 384.