SACRALISATION OF LUMBAR VERTEBRAE OR LUNBO SACRAL JOINT : Mukesh Goyal *
Abstract :
Background: Lumbar backache is a very common problem nowadays. Sacralisation of lumbar vertebrae is one of the cause for that. During routine osteology teaching a sacrum with incomplete attached lumbar 5 vertebrae is seen.
Observation: Incompletely fused L 5 vertebrae with sacrum is seen. The bodies of the vertebrae are fused but the transverse process of left side is completely fused with the ala of sacrum.But on the right side is incompletely fused.
Conclusion: The person is usually asymptomatic or may present with symptoms which include spinal or radicular pain, disc degeneration, L4/L5 disc prolapse, lumbar scoliosis and lumbar extradural defects. In transitional lumbosacral segmentation, it was observed that the lumbosacral intervertebral disc is significantly narrowed. The incidence of disc herniation is found to be higher and can occur even at young ages. There was also relationship established between transitional vertebrae and the degree of slippage in spondylolytic spondylolisthesis. In addition, this anomaly has known implications in the field of disc surgery.
KEYWORDS: Radicular Pain, Scoliosis, Herniation, Spondylolytic.
INTRODUCTION
In modern life backache is common complaint. Low back pain (LBP) is quite a common ailment affecting about 80% of the population in their life time [1]. One of the causes is sacralization of lumbar vertebra. Lumbosacral transitional vertebrae (LSTV) occur as a result of congenital anomaly in the segmentation of the lumbosac- ral spine. LSTV includes either the involvement of L5 in sacrum or S1 into the lumbar vertebrae. Sacralization means addition of sacral elements by the incorporation of Fifth lumbar vertebra. The incorporation of the fifth lumbar vertebra with the sacrum may be unilateral or bilateral producing partial or complete sacralisation. Complete sacralization consists of complete bony union between the abnormal transverse process and the sacrum. Incomplete sacraliza- tion shows a well defined joint line between the process and the sacrum.
Bertolotti 1st observed the LSTV and stated that these abnormal verte- brae may produce low back pain due to arthritic changes which occur at the site of false articula- tion[2]. LSTV are common with the prevelance ranging from 1-20% [3, 4]. Some previous workers have suggested the role of LSTV in low back pain [5, 6], whereas others have contra- dicted the role of LSTV [6,7]. This case is been highlighted to help clinicians to rule out LSTV/ sacralisation while diagnosing a case of low back pain.
CASE REPORT
During routine study of osteology in the Department of Sriganganagar College of Allied Health Sciences, Tantia University, Sri Ganganagar a sacrum with partial fusion of Lumbar 5 vertebrae was seen. The case is of sacralisation of lumbar vertebrae or LSTV.
OBSERVATIONS
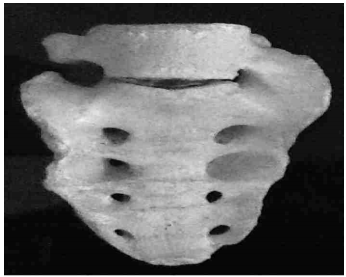
The body of the sacrum and L5 not fused but the transverse process on left side was completely fused and on right side not fused.
Measurement of vertical length of Lumbar 5 vertebrae 5.0 cm
Measurement of distance between transverse processes of L5 vertebrae- 5.7cm
Measurement of vertical and transverse diameter of intervertebral foramina-
Left- 1.5cm and 0.6cm Right- 1.5cm and 1.65cm
Fig. 1: Showing Sacralisation of Lumbar Vertebrae
Fig1 :
DISCUSSION
To understand the LSTVor sacralisation, we need to know the embryological origin of lumbar vertebrae. It commences at 3rd week of intrauterine life. All vertebrae originate from somites that form along the cranial-caudal axis, on either side of the notochord, from presomatic mesoderm. These somites differentiate further into dermomyotome (future inner dermis and muscle) and sclerotome. Each sclerotome consists of loosely packed cells cranially and densely packed cells caudally. Some densely packed cells move cranially opposite the center of myotome where they form intervertebral disc .
The remaining densely packed cells fuse with the loosely arranged cells of immediately caudal sclerotome to form mesenchymal centrum, body of vertebra. The mesenchyamal cells surrounding the neural tube form neural arch. Ossification of vertebra begins in 8th week & ends by 25th year. There are two primary centers & fi v e s e c o n d a r y c e n t e rs p r e s e n t i n e a c h vertebra[8].Secondary centers are one for the tip of spinous process, one for the tip each transverse process & two each for annular epiphyses. The primary cause of LSTV is cranial shifts that mean sacralization of the last lumbar vertebrae & partial shifts which mean unilateral fusion of the transverse processes. Literature is unclear about exact origin of LSTV; it is likely a product of both genetic predisposition (Hox gene product concentration) and developmental influences.Various studies have been done to find out the causes, incidence and clinical features of sacralisation of lumbar vertebrae. Kharinar and Nachale found 6.6% of cases in their study[9]. Which Correlate with the observations done by Chet Savage(7%, 2005)[10]. Magora and Schwartz found 20.8% sacralization in his study[11]; Sacralization was found in 11.1% cases by Kubavat dharati et al [12].Peter et al reported 6.2% sacralisation[13]. Otani et al. stated that a lumbosacral transitional vertebra was found more often in patients with disc herniation (17%) than in the control group(11%)[14].
The person is usually asymptomatic or may present with symptoms which include spinal or radicular pain, disc degeneration, L4/L5 disc prolapse, lumbar scoliosis and lumbar extradural defects [15]. In transitional lumbosacral segmentation,it was observed that the lumbosacral intervertebral disc is significantly narrowed[16,17,18].The incidence of disc herniation is found to be higher and can occur even at young ages [19,20,21].There was also relationship established between transitional vertebrae and the degree of slippage in spondylolytic spondylolisthesis [22]. In addition, this anomaly has known implications in the field of disc surgery. There are reports of surgery being performed at the wrong lumbar level [23] and the presence of a transitional vertebra may contribute to this error. It has been demonstrated that the discs immediately above the transitional vertebra were significantly more degenerative (disc protrusion or extrusion) compared with the disc found between the transitional vertebra and the sacrum [24,25]. Also, nerve root canal stenosis has been found at the level suprajacent to the transitional vertebra [24]. According to Castellvi et al. the transitional vertebrae cause abnormal torque movements above these anomalous vertebrae, a fact that could result in disc degeneration [26]. Aihara et al. in an anatomical study of 70 cadavers claimed that the iliolumbar ligament at the level immediately above the transitional vertebra is much thinner and weaker than in cadavers without a lumbosacral transitional vertebra[25].
LSTV therefore may be one of the causative factors for low back pain and the importance of its identification in patients with low back pain cannot be ignored. Complications of sacralization of 5th lumbar vertebra causes pain are actual pressure on nerves or nerve trunks, ligamentous strain around the sacralization, compression of soft tissues between bony joints, by an actual arthritis if a joint is present, by a bursitis if a bursa is present. Failure to recognize & to find LSTV during spinal surgery may have serious complications. LSTV is associated with disc herniation, sciatic pain in some individuals. During delivery of baby, pelvis fails to expand in sacralization.
Pain erupts 1st time in young age & frequently history given is pain for few years. The improper formation and union of somites can cause vertebral abnormalities, including block vertebrae, cleft vertebra, and unilateral and bilateral hemivertebrae[27]. Lumbar spine experiences more abuse from normal functions than any other part of human skeleton[19,20]. According to M.U. Eyo et al to be able to give support to and bear the weight of the body, the integrity of all the vertebrae in the spine, particularly in the lower back must be maintained[28, 29].
Conflicts of Interests: None REFERENCES
[1]. Dullerud R: Diagnostic imaging in lumbago and sciatica . Ugeskr Laeger 1999, 161: 5299-303.
[2]. Bertolotti M:Contributoallaconoscenzadeivizi di d i f f e r e n z a z i o n e r e g i o n a l e d e l r a c h i d e conspecialeriguardo all assimilazionesacraledella v. lombare. Radiol Med., 1917;4:113-144.
[ 3 ]. Ca st e ll v i AE, Go l d st e i n LA, Ch a n DPK:Lumbosacral transitional vertebra and their relationship with lumbar extadural defects. Spine 1983, 9:493-495.
[4]. Vergauwen S, Parizel PM, Van Breusegem L, VanGoethem JW, Nackaerts Y, Van den Hauwe Letal: Distribution and incidence of degenerative spine changes in patients with a lumbosacral transitional vertebra. Eur Spine J. 1997, 6(3):168- 172.
[5]. Quinlan JF, Duke D, Eustace S:Bertolotti’s syndrome. Acause of back pain in young people. J Bone Joint Surg (Br) 2006,88(9): 1183-1186.
[6]. Bonaiuti D, Faccenda I, Flores A:Sacralisation of the 5th lumbar vertebra and backache: what’s the possible relationship? Med Lav.1997, 88(3): 226- 236.
[7]. Southwood JD, Bersack SR: Anomalies of the lumbosacral junction in 550 patients without symptoms referable to the low back. AJR 1950,64:624-634.
[8]. Moore KL, Persaud TVN: From The Developing human: clinically oriented embryology. In S k e l e t a l s y st e m . 8 t h e d , S a u n d e rs, Elsevier,Philadelphia ;2008: 344-346.
[9]. Khairnar KB, Rajale MB. Sacralisation of Lumbar Vertebrae. Indian Journal of Basic & Applied Medical Research; March 2013: Issue-6, Vol.-2, P. 510-514
[10]. Chet Savage. Lumbosacral Transitional Vertebrae: Classification Of Variation and Association with Low Back Pain A Thesis presented to the Faculty of the Graduate School University of Missouri-Columbia; July: 2005.
[11]. Magora A, Schwartz A. Relation between the low b a c k p a i n s y n d r o m e a n d X – r a y findings.Transitional vertebra (mainly sacralization) Scan J Rehabil Med 1978, 10: 135- 45.
[12]. Kubavat Dharati, Nagar S K,Malukar Ojaswani ,Trivedi Dipali,Shrimankar Paras,Pati l Sucheta:National journal of medical research , Vol.2(2), apr-june2012.
[13]. Peter H.Wilm B,Sakai N,Imai K,Maas R,Balling R:Pax 1 & Pax 9 synergistically regulate vertebral column Development 1999,126: 5399-408.
[14]. Otani K, Konno S, K ikuchi S; Lumbosacral transitional vertebrae and nerve-root symptoms. JBone Joint Surg. (Br) 2001, 83(8):1137-1140.
[15]. Williams, P. L.; Warwick, R.; Dyson, M. & Bannister, L. H. Gray’s Anatomy. 37th ed. New York, ELBS- Churchill Livingstone,1989.
[16]. Tini, P. G.; Wieser, C. & Zinn, W. M. The transitional vertebra of the lumbosacral spine: its radiological classification, incidence,prevalence and clinical significance. Rheumatol. Rehabil. 1977,16(3):180- 5.
[17]. Ebraheim, N. A.; Miller, R. M.; Xu, R. & Yeasting, R.A. The location of the intervertebral lumbar disc on the posterior aspect of the spine. Surg. Neurol. 1997, 48(3):232-6.
[18]. Revuelta, R, De Juambelz P P, Fernandez B and Flores J A.Lumbar disc herniation in a 27-month old child. Case report. J. Neurosurg. 2000, 92(1):98- 100.
[19]. Williams, PC. The lumbosacral spine, emphasizing conservative management. New York, McGraw-Hill Book Company 1965,27-32.
[20]. Williams, PC. The lumbosacral spine, emphasizing conservative management. New York, McGraw-Hill Book Company 1965, 149- 50.
[21]. Otani K, Konno S ,K ikuchi S. Lumbosacral transitional vertebra and nerve root symptoms. J. Bone Joint Surg. Br. 2001,83(8):1137-40.
[22]. Kim NH & Suk KS. The role of transitional vertebrae in spondylolysis and spondylolytic spondylolisthesis. Bull. Hosp.Jt. Dis.1997, 56(3):161-6.
[23]. Wiese M, Krämer J, Bernsmann K , Ernst Willburger R. The related outcome and complication rate in primary lumbar microscopic disc surgery depending on the surgeon’s experience: comparative studies. Spine J.2004, 4(5):550-6.
[24]. Vergauwen S, Parizel PM, Van Breusegem L, Van Goethem JW, Nackaerts Y, Van den Hauwe Let al.; Distribution and incidence of degenerative spine Distribution and incidence of degenerative spine changes in patients with a lumbosacral transitional vertebra. Eur Spine J., 1997; 6(3):168-172.
[25]. Aihara T, Takahashi K, Ogasawara A, Itadera E, Ono Y, Moriya H; Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: a clinical and anatomical study.J Bone Joint Surg Br., 2005; 87(5):687-691.
[26]. Ca st e l l v i AE, Go l d st e i n LA, Ch a n DPK:Lumbosacral transitional vertebra and their relationship with lumbar extadural defects. Spine, 1983; 9:493-495.
[27]. Schmorl G and Junghanns H.:The human spine in health and disease (2nd American Edition) Edited and translated by Besemann EF. New York: Grune & Stratton. 1971.
[28]. Eyo MU , Olofin A, Noronha C, Okanlawon A: Incidence of Lumbosacral Transitional Vertebrae in Low Back Pains, PatientsWest African Journal of Radiology , April 2001: 8(1).1-6
[29]. Ravindra Kumar Boddeti, Gargi Soni, Pradeep Kumar H Murudkar. Lumbosacral Transitional Vertebra: A Case Report. Sch J Med Case Rep 2014; 2(1):1-2.