EFFECT OF SNAGS TECHNIQUE ON HEART RATE AMONG PATIENTS WITH UPPER CERVICAL DYSFUNCTION : Mitali Badulkar * Maneesh Arora ** Parul Raj Agrwal ***
ABSTRACT
Background: Mulligan’s mobilization techniques are thought to increase the range of motion as well as correct the alignment of spine. The aim of this study was to investigate the effect of SNAGS technique on heart rate among patients with upper cervical dysfunction with vagus nerve impingement.
Need of the study: To best of our search there is dearth of literature pertaining to the involvement of vagus nerve at the upper cervical complex dysfunction and thus its effect on heart rate. Methodology: 80 subjects were taken on the basis of inclusion- exclusion criteria in this study. Pre intervention heart rate was recorded .SNAGs technique was given to the patient’s atlas vertebrae to side it was stuck. Post intervention heart rate was noted.
Result: The data was analysed using SPSS version 16. Descriptive statistics was used to summarise the variables. Paired T Test was used to see the effects of intervention on heart rate in our study population. There was reduction in heart rate by 5.2 beats/min which was found to be statistically highly significant (p ? 0.001).
Conclusion: The study concluded that SNAGS technique was effective in correcting the impingement caused to vagus nerve as measured through HR in patients with upper cervical dysfunction.
Key words: Cervical dysfunction,Vagus nerve impingement, Heart rate, Heart rate alteration.
INTRODUCTION
Cervical spine dysfunction
The cervical spine dysfunction is a common condition. It is represented by a group of signs and symptoms that involve pain and limitation of range of the physiological movements, tenderness and/or pain on cervical muscles at palpation.
There is a variety of reasons for cervical spine pain apart from obvious trauma or a history of trauma. These include mainly postural or degenerative causes. An increasing proportion of the population spend long periods sitting or in sustained positions. This occurs in both the work and social environment which in fact, is creating an increase in these types of conditions seen, specifically in the younger and more sedentary population.
Conditions under upper cervical dysfunction are cervical spondylosis, Neck pain as a result of forward head posture which could also lead to Cervicogenic 1 headaches , Prolapsed intervertebral disc, Muscle 4 imbalances and trigger points , Vertigo etc.
Cervical spine dysfunction may lead to misalignment most commonly of upper cervical joint complex especially the atlas. Many vital structures pass through the upper cervical joint complex, upper cervical joint complex, one of the most important being the vagus nerve. Vagus nerve exits the skull through the jugular foramen and passes vertically down the neck within the carotid sheath, lying between the internal jugular vein and internal carotid artery as far as upper border of thyroid cartilage, and then between the same vein and common carotid artery until it reaches the roof of the neck. In the neck the vagus gives cardiac branches, two or three in number from superior and inferior cervical 2 levels. the vagus provides heart with its parasympathetic supply.
Thus any misalignment of atlas vertebra in the upper cervical joint complex leads to effect on vagal action which consequently does not carry out its function of antagonist to the sympathetic system properly, causing increased heart rate, also painful stimuli is carried by unmyelinated ‘c’fibers to synapse with pressor area of ‘vasomotor cortex’ therefore, their activation causes sympathetic stimulation producing tachycardia and rise in BP. Normal heart rate for an adult is 70 – 80 beats 3 / min.
Cervical spine pain is a common ailment seen these days. Medically, this is often diagnosed by radiography and treated with anti-inflammatory medication. While medication assists in short term pain relief, symptom relief, and masking of pain, it does not address or treat the underlying causes of cervical spine dysfunction. Therefore numerous techniques such as muscle energy techniques, chiropractic manipulation, Maitland mobilization, stretching, and myofacial release, kneeding, SNAGS, NAGS, MWM’S, traction etc. have now been developed for correction of misaligned spine. SNAGS is technique which first distracts (opens) and then compresses (closes) the zygapophyseal joint ipsilateral to the side of pain, and perhaps slightly distracts the uncovertebral cleft.
The therapist applies the appropriate accessory zygapophyseal glide while the patient performs the symptomatic movement. This must result in full range pain free movement. SNAGs are most successful when symptoms are provoked by a movement and are not multilevel. They are not the choice in conditions that 6 are highly irritable. Although SNAGs are usually performed in weight bearing positions they can be 7 adapted for use in non-weight bearing positions.
To best of our search there is dearth of literature pertaining to the involvement of vagus nerve at the upper cervical complex dysfunction and thus its effect on heart rate. Impingement of vagus nerve due to misalignment of atlas vertebrae can also influence the function of Gastro Intestinal system and Cardio Vascular systems affecting the Heart Rate so, upper cervical complex evaluation for impingements should also be considered while looking for dysfunctions related to Heart Rate caused by decreased vagal tone.
METHODOLOGY
This study is an experimental study to determine the effect of SNAGS Technique on HR among patients with upper cervical complex dysfunction. The study was conducted in the various opd’s of private institute in Dehradun. All subjects between the age limits 20 – 60 years visiting the opd’s were taken in the study. Simple random sampling was done. Participants with cervical spine dysfunction who were in age group 20- 60 years of either gender with Any dysfunction of cervical spine due to rotation of C -C vertebras and 1 2 were willing to participate were included in the study. Patients with any cardiac conditions which may alter the heart rate, Fractures of the cervical spine, Any acute muscle pathology. (e.g. Strain ),Any diagnosed medical or surgical condition in which SNAGS technique cannot be used, Systemic diseases affecting the vertebral column preferably cervical spine (e.g. Infections),Patients having vertigo problem and Uncooperative patients were excluded from the study.
SNAGs TECHNIQUE:
This technique is extremely useful in restoring upper cervical rotation and especially when manipulation is contraindicated.
The patient is seated and the therapist stands behind him. The therapist placed the pad of his thumb on the transverse process of the atlas vertebra on the opposite side of restricted rotation and it is superimposed by his other thumb. The patient is then asked to slowly rotate his head to the restricted side as the therapist provides a gliding force ventrally on C1 with his thumb to assist the movement. The thumb pressure is not released until the neck returned to midline. The patient must feel no 7 pain.3 sets of 8 repetitions are performed.
Prior to starting of the study, ethical approval was taken. 130 subjects were screened in the earlier phase of HR study.80 subjects participated in the study based on inclusion and exclusion criteria.Procedure was explained in detail to the participants, following which the written informed consent was taken .Patient was made to relax for 5 mins so that anxiety factor doesn’t influence the HR reading. Motion palpation was done for cervical vertebrae to check the side of the stuck atlas (C1) vertebra . Pre intervention heart rate was recorded. SNAGs Technique was given to the participants on their affected side. Post intervention heart rate was measured within 1 min of the treatment. Data recorded and analysed.
DATAANALYSIS:
The data was analysed using SPSS version 16. Descriptive statistics was used to summarise the variables. Paired T Test was used to see the effects of intervention on heart rate in our study population. p value < 0.05 was considered significant.
RESULT:
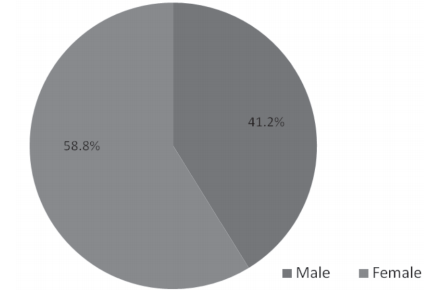
Mean age of participant was 35.5 years (SD±12.2).The gender distribution in our study was, 41.2% male and 58.8% were female participants.
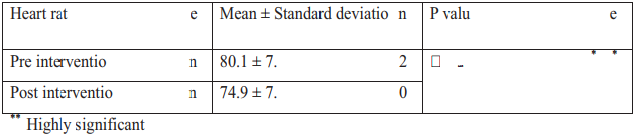
The mean Heart rate of the participants before the intervention was 80.1 ± 7.2 beats/min and after the intervention the mean heart rate recorded was 74.9 ±7.0 beats/min (table 1).There was reduction in heart rate by 5.2 beats/min which was found to be statistically highly significant (p ? 0.001).
Table 1 Showing change in heart rate following SNAGS technique:
In our present study mean age of participant was 35.7 ± 12.2 years. 41.1% of participants were male and 58.8% were females (fig 3).
FIGURE 3 – Showing gender distribution of the participants
DISCUSSION
This study was designed to check the effect of SNAGs technique on heart rate among patients with upper cervical dysfunction with vagus nerve impingement.
The study was conducted on 80 participants with cervical dysfunction. The mean age of the participants was 35.7±12.2 years, in which there were 41.1% males and 58.8% females. In the present study the numbers of females were more as compared to males with cervical dysfunction. This was similar to study conducted by Wendy Rheault,Chris Byers et al where author reported higher distribution of female population with cervical dysfunction. The purpose of this study was to investigate the intertester reliability of the cervical range of motion device (CROM). The CROM was used to measure subjects with a history of cervical dysfunction. The sample consisted of 22 subjects (15 8 female and 7 male).
This could be because most of the females are usually involved in task requiring less physical work thereby promoting their sedentary lifestyle which is reported one of the contributory factor for cervical 9 dysfunctions. One of the many reasons for cervical spine dysfunction in females could be due to the misalignment of cervical and thoracic curveswhich could be result of faulty postures developed in females from their early adolescence due to breast development 10 and joint laxity thus inclining their posture towards relative thoracic kyphosis leading to compensatory changes in the cervical spine resulting in forward head 11,12 posture and neck pain.
In addition to above reason Geertje A.M. ArieÈns, Willem van Mechel, Paulien M. Bongers et.al also studied that neck pain could also be associated with psychological risk factors. However the psychological factors were not learnt in our study. The recent prevalence data showed that in a general population the 1 year prevalence of neck pain was 15% and 17% of 13,15,17 males and females respectively. The prevalence data in occupational setting was even more impressive. Skov et al. (1996) reported 1 year prevalence of neck pain in sales people (n=1304) with females being 18 predominant.
In our study the mean baseline heart rate of participants was 80±7.2 beats/min which was towards 3 the higher side of normal range of heart rate .literature revealed the neck pain can influence the sympathetic activity. As all the participants in our study had symptomatic increased neck pain which could have influenced the baseline HR of the participants.
Following SNAGS technique, in our study there was a reduction in heart rate by5.2 beats/min which was highly significant (p? 0.001) statistically. This decrease in heart rate could be due to reduction in pain which was noted following correction of misaligned spine. Abid Ali, Syed Shakil-ur-Rehman, and Fozia SibtainEt al reported in study which was done on 102 patients of non specific neck pain that SNAGS technique was very effective with isometric exercises 19 training of the neck .
Other reason for HR reduction could be misalignment or the atlas vertebra being rotated causing impingement of the vagus nerve passing on either side of the upper cervical complex. This impinged vagus nerve on the side of rotated atlas can cause various dysfunctions in the gastrointestinal 2 system, cardiovascular systems etc due to reduction in the parasympathetic action of the nerve. This decrease in the parasympathetic action cannot be noted by checking the direct action of vagus on the viscera’s of our body .This is where the cardiovascular system comes in place. The heart rate is regulated by constant parasympathetic action of vagus on the heart, called 16 vagal tone . when vagus gets impinged in the upper cervical complex; it causes decrease in the parasympathetic action of vagus on the heart causing increase in heart rate.
In our study the cervical misalignment was corrected via SNAGS technique. As compared to other technique SNAGS can be given in sitting or standing which has real advantage. When improvement takes place in functional posture they are more likely to be 7 retained.
SNAGS is a pain free technique whereas other techniques like manipulations etc. are painful and can have serious complications if not done correctly and can cause increase in heart rate due to pain.
This shows that our intervention has resulted in significant reduction in heart rate which in turn affirms that the misaligned atlas can result in impingement of the vagus however the anxiety factor could not be measured. Also objective assessment of pain was not done.
Future scope of the study can be that the heart rate could be measured within 5 min and 10 min to check the long term effect of the intervention, More objective assessment could be used for checking rotation of C1vertebra, Joint range of motion of Cervical spine can also be measured.
Conclusion:
The present study concluded that SNAGS technique was effective in correcting the impingement caused to vagus nerve as measured through Heart Rate in patients with upper cervical dysfunction.
REFERENCE
1. Page P. Sep 2011. Cervicogenic headaches: an evidence led approach to clinical management. international journal of sports physical therapy ;vol 6(3):254-256
2. P e t e r L. Wi l l i ams (DSC, MA, MB, FRCS).1995,gray’s anatomy, 38edition, Churchill Livingstone.
3. Jain A.K, 2012. Textbook of physiology. 5edition. avichal publishing company; vol 1:349- 357
4. Jaeger, B. (1989). Are “cervicogenic” headaches due to myofascial pain and cervical spine dysfunction. Cephalalgia, 9: 157–164.
5. G. zito et.al. May 2006. Clinical tests of musculoskeletal dysfunction in the diagnosis of cervicogenic headache. manual therapy; Vol 11, ( 2): 118–129
6. A. Hearn ,D.A. Rivett. May 2002,Cervical SNAGs: a biomechanical analysis. Elsevier. Vol 7 (2):71- 79.
7. Manual therapy NAGS,SNAGS,MWMS,etc by Brian R.Mulligan, 6th edition, 2010
8. Wendy Rheault, Geertje A.M. ArieÈns, Willem van Mechelen, Paulien M. Bongerset .al. 1992. Intertester Reliability of the Cervical Range of Motion Device Journal of Orthopaedic & Sports Physical Therapy; Vol:15(3):147–150
9. Mfrekemfon P. Inyang et .al. Apr2015.Sedentary Lifestyle: Health Implications. Journal of Nursingand Health Science ;Vol 4(2): 20-25
10. Carmen E. Quatman et.al. June 2008. The Effects of Gender and Maturational Status on Generalized Joint Laxity in Young Athletes. J sci med sport ; vol11(3):257 263
11. Quek J et.al, Feb. 2013. Effects of thoracic kyphosis and forward head posture on cervical range of motion in older adults. manual therapy; vol18 (1):65-71
12. Black, Kathleen et.al. Jan 1996. The Influence of Different Sitting Positions on Cervical and Lumbar Posture. spine ; vol21 (1):65-70
13. Lau EMC, Sham A, Wong KC. 1996. The prevalence of and risk factors for neck pain in Hong Kong. J Pub Health Med 18:396-399.
14. Raj Rao, MD.2002 Oct. Neck Pain, Cervical Radiculopathy, and Cervical Myelopathy Pathophysiology, Natural History, and Clinical Evaluation, J Bone Joint Surg Am; vol 84 (10): 1872 -1881
15. Hooftman, Wendela E et.al. March 2005. Gender Differences in Self-Reported Physical and Psychosocial Exposures in Jobs With Both Female and Male Workers, Journal of Occupational & Environmental Medicine;Vol47( 3) : 244-252
16. Jain A.K, 2012, textbook of physiology, 5edition, avichal publishing company, vol1 :333- 345
17. Geertje A.M. ArieÈns, Willem van Mechelen, Paulien M. Bongers et.al. Psychosocial Risk factors for neck pain: a systematic review. American journal of industrial medicine; vol39:180-193.
18. Skov T, Borg V, érhede E. 1996. Psychosocial and physical risk factors for musculoskeletal disorders of the neck, shoulders, and lower back in salespeople. Occup Environ Med; 53:351-356
19. Abid Ali, Rehman, Fozia. 2014 Jul-Aug The efficacy of Sustained Natural Apophyseal Glides with and without Isometric Exercise Training in Non-specific Neck Pain. Pak j med sci.; vol 30(4): 872–874.