“TO CHECK THE RELIABILITY AND CONCURRENT VALIDITY OF A NEW METHOD FOR TESTING THE LENGTH OF TENSOR FASCIA LATAE” : Sumeeta Khaund Grover *
Background
Few investigations include both strengthening and proprioceptive exercises in the treatment of bilateral knee osteoarthritis. Though previous studies give us some insight in to the role of individual strengthening and exercise proprioceptive exercises in knee OA but none of the studies have studied the combined effect of strengthening exercises and proprioceptive oxercises in knee OA. Thus, it is intended to check the efficacy of proprioceptive and strengthening exercises in knee OAto reduce pain and functional disability and improve joint position sense.
Methods
In this study 24 subjects who met the inclusion criteris were randomized into three groups three groups. Group Awere given conventionzl treatment (SWD and static quadnceps). Group B were given strengthening exercises along with SWD. Group C; which were given strengthening exercises and proprioceptive exercises along with SWD. Outcome measures were pain, functional disability and joint position sense.
Results
All the groups significantly improved in VAS and WOMAC scores after intervention po. 05, knee reposition error score (joint position sense) only improved in proprioceptive exercises group. The proprioceptive exercises group demonstrated greater improvement in VAS and WOMAC scores as compared to other two groups.
Conclusion
This study between three groups comparing proprieceptive treatment to strengthening and proprioceptive exercises suggest that combination of the two brings.
Study Design
The study was a randomized controlled trial.
Objective
To compare the effectiveness of proprioceptive exercises and strengthening exercises and combination of two along with short wave diatheramy in treatment of osteoarthritis of knee in terms of pain and functional disability.
Background
Few investigations include both strengthening and proprioceptive exercises in the treatment of bilateralknee osteoarthritis. Though previous studies give us some insight in to the role ofindividual strengthening and exercise proprioceptive exercises in knee OA but none of the studies have studied the combined effect of strengthening exercises and proprioceptive oxercises in knee OA. Thus, it is intended to check the efficacy of proprioceptive and strengthening exercises in knee OA to reduce pain and functional disability and improve joint position sense.
Methods
In this study 24 subjects who met the inclusion criteris were randomized into three groups three groups. Group A were given conventionzl treatment (SWD and static quadnceps). Group B were given strengthening exercises along with SWD. Group C; which were given strengthening exercises and proprioceptive exercises along with SWD. Outcome measures were pain, functional disability and joint position sense.
Results
All the groups significantly improved in VAS and WOMAC scores after intervention po. 05, knee reposition error score (joint position sense) only improved in proprioceptive exercises group. The proprioceptive exercises group demonstrated greater improvement in VAS and WOMAC scores as compared to other two groups.
Conclusion
This study between three groups comparing proprieceptive treatment to strengthening and proprioceptive exercises suggest that combination of the two brings better rellet to the subjects of knee OA in reducing pain and functional disabllity.
Introduction
Osteoarthritis (OA) is the most common joint disorder, a prevalence that increases with age and sex specifications”. Among adults 45-74 years of age or older. symptomatic disease occurs in approximately 12.1 % population’ Before 50 years of aoe the provalence of OA in most joints is higher in men than in women. After about 50 years of age, women are often affected with hand, foot and knee OA than men3In subjects with no joint pain who have radiographic changes of OA. quadriceps weakness predicts radiograph progression and pain”. These findings suggest that the weakness may occur before arthritic damage.
Nevertheles, exercises to strengthen the quadriceps relieve joint pain in persons with OA of knee’. the strangthaning exercises are beneficial for knee OA by several pathways. improving strength. improving psychological well-being. All of these may interact and have an additive effect on the symptoms of OA’. Barret et al. (1991) has reported impaired proprioception for the patilents sullering from knee osleoarthritis. Few investigations have investigated the relationship between impaired proprioception and performance or other measures of functional status in OA. In addition Birrninghsm et al. (2001) stated that quadriceps sensory dystunction that is, decreased proprioceptive acuity. has recently been demonstrated in patients with knee OA and proposed as a factor in the pathogenesis or progression of the condition. If correct, restoration of these sensorimotor deficits with strengthening may retard progression of knee OA and reduce disability. Although it is generally accepted that a rehabilitation program improves the functional capacity, pain and sensoriomotor function of patients, there is lack of agreement about what such a rehabilitation program should include (Roddy et al. 2005). Many previous studies have generally used sophisticated and expensive apparatus. Which limits their application to a community setting”10. Though the above mentioned studies give us some insight in to the role of proprioceptive exercises in knee OA but none of the studies have studied the combined effect of strengthening exercises and proprioceptive exercises in knee OA. Thus, in this study it is intended to check the efficacy of proprioceptive and strongthening exercises in knee OA to reduce pain, functional disabllity and improve joint position sense.
Patlents and Methods
Under convenience sampling, 30 subjects were recrulted from the physlotherapy department of in Udaipur hospitals and. The subjects were screened by means of a screening form one of the three groups-group A proprioceptive treatment group). group B (strengthening exercise treatement group) and group C (strengthening exercise and proprioceptive exercise) by simple randomization method.
Inclusion Criteria
1. Diagnosed cases of osleoarthritis grade 2 and 3 (As reported by radiologist).
2. Age group 45-60 years
3. Bilateral osteoarthritis.
4. Gender post meno pausal
female Exclusion criteris
1. Neurologic disorder (e.g. parkinson’s disease, Alzheimor’s disease)
2. Steroid injection in past 2 months
3. Infiammatory arthritis
4. Metal implants in lower limb
5. Osteoporosis
6. Knee ligament/Meniscal injury
Group A received short wave diathermy and static quadriceps exercise, Group B received short wave diathermy and strengthening exercises and Group C received short wave diathermy and strengthening exercises and Group C recelved short wave diathermy. strengthening exercises and proprioceptive exercises.
Intervention
1. Before starting the exercises, patients were given treatment for pain reduction by Diatheramy diathermy. The patients were positionedsupine and comfortably on the treatment plinth. Patient in each groupreceived 20 min of SWD thrice a week for four weeks (12 treatments) applied by malleable electrodes by contraplanar method (chitra, 2007)”. The intensity of the SWD was based on each subject’stoferance but all the subjects were advised that they should feel justcomfortable warmth (Low and Reed, 2000).
2. Strengthening exercises (Gail D, 2005)” Static quadriceps in knee extension- Patient is positioned fully supine. Patient contracts the quadriceps femoris muscle and pushes knee down while maintaining the fool in full dorsiflexion, each contraction is held for 6 sec with a 10 sec rest between repetitions. 10 repetitions are done.
Standing terminal knee extension- Patient stands with a resistive band behind a slighthy flexed knee. Patient contracts the gluteal and quadriceps femoris muscle to fully straighten the hip and knee. Each contraction is held for 3 seconds, 10 repetitons were done and resistance is increased as tolerated by the patient.
Closed chain exercise, one of the two exercises is performed 3 times per week. Patiend should progress to tha most challenging activity that he or she can successfully complete with minimal or no pain.
a. Seated leg press-Patient is seated holding a resistive band in both the hands :
A patient places his or her foot aginst the band, then straightens the knee by straightens the knee by pushing the foot down and forward by contracting the gluteal and quadriceps femoris muscles. Each contraction is helf for 3 seconds with knee as straight as possible,patient slowly return to the starting position and repeat for 30 sec bout.Progression is made by using bands of high resistance and additional bouts.
b. Partial squats-patient stands with arm support as needed, patient performs a partial squal, keeping the knees centered over the feet return to standing by contracting the quadriceps femoris and glutealmuscles. Each contraction is held for 3 seconds with hips and knees as straight as possible. Progress to full body weight without support andadditional bouts.
3. Proprioceptive exercises. (chita et al. 2007)”
a. One leg balance-it involed standing on affected foot with relaxed upright posture and other leg flexed at knee. hip and ankle, this position was held for one minute followed by rest for 10 to 20 seconds and was repeated twice more After a brief rest three similar repetitionswere carried out for unaffected leg (Fig a).
b. Blind advanced one leg balance-it was same like one log balance,expect that the patient was asked to keep his/her eyes completelyclosed while performing the routine, and then was repeated twice again(Fig b).
c. Toe walking-Here the patient was made to walk for 20 meters high up on the toes with loes pointing straight ahead, then walk with toes pointingstraight ahead. then walk with toes pointing outwards and thenwalk with toes pointing imwards after a short rest repeat it once again(Fig C)
d. Heel walking-Walking for 20 meters on heels with toes pointing straight ahead, walking on heels with toes pointing out and walking on heels with toes pointing in. After a short rest, the procedure wasrepeated once more (Fig d)
e. Gross leg body swing-Leaning slightly forward with hands on wall for support and weight on affected leg. other leg was swung in front of the body pointing toes upwards as foot reaches its farthest point of motion. Then swing this unaffected leg back to the unaffected side as faras comfortably possible, again pointing toes up as foot reaches its final point of movement. Repeat this overall motion 15times with erect body posture and good balance, rest for a few seconds, and then 15 similar repetitions with the unaffected leg as weight-bearing limb was performed (Fige)
Treatment was given three times per week for four weeks. In this study the outcome measures were- :
All outcome measures were measured at baseline, end of week 1. end of week 2. end of week 3 and end of week 4.
Pain-was measured using the visual analoguo. Functional disability-was measured using the Western Ontario and McMaster Universitios Osteoarthritis Index (WOMAC) Joint position sense-was measured using inclinometer by Reposition error test (Higgins and Perrin, 2000)
Procedure for reposition error test-all the subjects were familiarized with the procedure by explanation, demonstration and adequate practice repetition. Inclinometer was attached to the distal thigh of dominant extremityapproximately one inch above knee joint line. Patient is standing with back against wall and is blindfolded to eliminate visual coes, Patient squats to 30 degree of knee flexion and maintains this position for 15 sec, return to starting position of 0 degree extension, Following a 15 sec rest period patient then attempts to repostition themselves at the predetermined angle, degree of error from 30 degree knee flexion target anlge is recorded and average over three trials is used for data analysis (Higgins and Perrin, 2000)13.
Inclinometer for assesing joint pasition sense (Reposition error lest)
Statistical Analysls
A Total of 30 patients were screened for possible study eligibllity. 28 patients satisfied the eligibility criteria, were recrulted into study and underwent baseline measurement. Four patients in this study did not complete the treatment. There were two dropouts from Group A, one each from Group B and Group C. Total of 24 subjects, includingfemales45. completed the study. Age of subjects in this study was between 60 years. The mean age of subjects in Group A was 51.5 (4.30) Years. Group B was 49.5 (+2.44) years, and Group C was 51.62 (+3.96) years. There was no significant difference between the mean ages of all the three groups. Group A had 8 females patients, Group B had 8 females GroupC had 8 female patients.
Readings of the variables taken at the baseline and at the end of first second, third and fourth week were analyzed for intragroup differences using repeated measure ANOVA and paired samples t-test with Bonfarroni correction. Intergroup differences were analyzed using one way ANOVA.
For intergroup differences result was considered significant if p value d 0.05 and for intragroup differences result was considered significant if p-valued 0.01.
Results
Within Group analysis of pain scores-The repeated measures ANOVA results for VAS scores revealed a significant difference within all groups.
Between group analysis of pain scores- The analysis of VAS scores Between all the groups suggested that there were no significant differences at the baseline (p=0.397) and at the end of 1st week (p=0.052) At the end of 2 nd week there was significant difference between the groups (p=0.002). at the end of 3rd week there was significant difference between the groups (p=0.000) , at the end of 4th week there was significant difference between the groups (p=0.000).
Within Group Analysis of WOMAC Scores. The analysis of WOMAC score between the groups suggested that there were no significant differences between baseline (p=0.110) and week 1 (p=0.467) At the end of 2nd week there was significant difference between the groups (p=0.003). At the end of 3rd week there was significant difference between the groups (p=000). At the end of 4 th week there was significant difference between all the groups (p=.000).
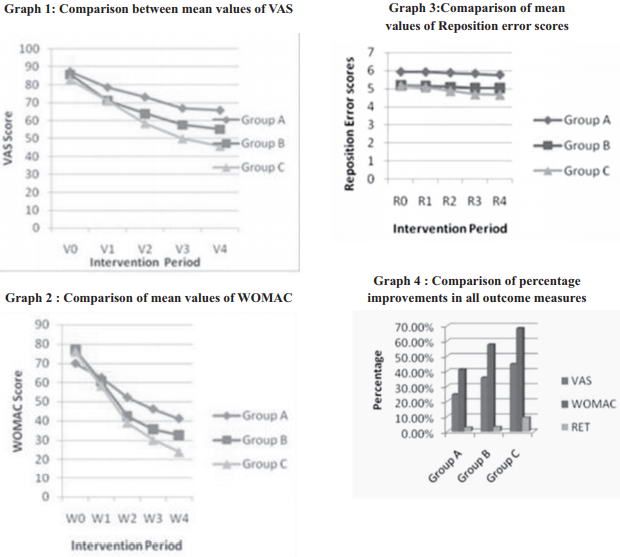
Within Group Analysis of Reposition Error Test acores- The results of repeated ANOVA and post-hoc ttest showed no significant differences in Reposition scores in group A and B. But in Group C there was statistically significant improvement in baseline and week 4.
Between Group Analysis of Reposition error testThe analysis of reposition error score between the groups suggested that there ware no significant differences between baseline (p=o.193). week 1 (p=0.144). week 2 (P=0.135), week 3 (P=0.095) and week 4 (P=0.113).

Discussion
The purpose of this study was to determins the effectiveness of Proprioceptive axarcises along with strengthening exercises in improving pain and disability in patients with knee osteoarthritis. In all the three groups-pain. disability and joint position sense were taken as the dependent variables to assess the improvement between the groups and within the group. The findings of the present study suggest that the addition of proprioceptive exercises and strengthening exercises reduces patient’s pain and disability more effectively than strengthening exercises or Proprioceptive physiotherapy alone over a 4 week period. Statistical analysis revealed no significant differences in key demographic variables and baseline measurements of pain, disability and active angle replication test suggesting that all the groups had homogenous distribution of patients.
In this study VAS was usaed to measure pain. A statistically significant difference was found between all the groups. Maximum reduction of pain was in group C (37×0.02mm). this is in favor of our research hypothesis.Pain relief in this group is inaccordance with a case report of 70 year old lady with osteoarthritis of knee who found moderate pain relief by proprioceptive exercises as done by childs et at (2002)”. Reduction in pain in Group a (Proprioceptive treatment) and B (strengthening exercise group) is consistent with previous findings which state that both dynamic and isomelnc resistance training reduced parceived knee joint pain” Proprioceptive training reduced parceived knee joint pain” Proprloceptive training activities provide patient with an opportunity to adapt to potentially destabilizing loads on the knee during rehabilitation. give additional exposure to pivoting, quick starting and stopping and quick changes in direction and challenge their balance capabilities. Strengthening exerclese are recommended to reduce pain and improve physical function in knee O.A., but there is minimal information on its long term impact. it is theorued that because elevated plasma a endorphin, a nauro transmitter inhibltory to pain signal, has been observed in response to prolonged rhythmic exercise (Thoren et al, 1990) leading to increased a eondorphin production might decrease pain experienced by persons with osteoarthritis”.
In the present study WOMAC score was used to asses overall knee lunction since its validity and reliability is already established” The analysis of disability score reveals no significant difference at baseline There was significant improvement in Group B (Strengthening exercises) and C (strengthening exercise and propricoceplive exercises) as compared to Group A (Proprioceptive treatment) but maximum difference in mean score of Group C (52 mm), supporting ourresearch hypothesis. Both the treatment groups A and B resulted in significant improvements in all the vartables compared to the Proprioceptive therapy group. A study by Folson et al (2009) states that proprioceptive acuity as assossod by the accuracy of reproduction of the angle of knee llexion has modest effects on pain and physical function limitation in knee osteoarthritis. This could be due to pain relial, reduction in stiffness. increased lubrication of joint, gain in strangth of weak muslces, correctmechanical loading. Improved joint stability and thus increased quality of movement and improved proprioception which in tum provides participants an opportunity to adapt to potentially destablizing load on knee during the study period”. Hurley at al (2004) have reported that proprioception is closely related to functional performance and walking speed. This is in accordanca with this study which shows greater mean difference in proprioceptive exercises group than with other two groups.
In the study joint position sense was measured by reposition error test (RET). The analysis of RET at basaline revaals no significant differences between all the three groups. At the end of 4th week mean differences were not significant between all the groups. There was improvement in all the groups which supports the study that proves general exercise training can increase proprioceptive pertormance (Bernauer at al. 1994) Maximum reducation in mean was in Group C (0.48*). The difference between the moderate improvement in other two groups as compared to Group C and greator improvament in this group was probably due to specific proprioceptive exerclses. Proprioceptive information along (without visual loodback) can correct up to 95* % of velocity and timing errors associated with sudden perturbation in resistance during a multi-joint movement sequence”
Group A propriociptive Group B (strengthening exercises) and Group C (Proprioceptive and strengthening exercises) does not show any statistically significant difference at the and of 4 week study period. This is in accordance with a study done by solor at al. 2005 in which 6 weeks of proprioceptive and balance training was given to treatment group while the control group did not receive any exercise but there was no significant differences by the end of training in weight baaring joint position sense. Therefore, it may be concluded that proprioceptive acuity takes longer duration to shoe significant improvement.
Sample size was small and data was collected from limited place that limits the generalizability of the results. The duration of study was short (4 weeks) therefore long term effectiveness of propriocaptive exercises was not avaluated. Neither the subjects nor the therapist were blinded to group assignment. The cohort of patients with knee osteoarthritis wre predominately female, hence generalizability of our findings may not necessarily be applicable to the entire population of individuals with osteoarthritis.
This study showed that patients affected with OA knee. When performed proprioceptive exercises along with strengthening exercises showed significant reduction in pain and functional disability and improvement in propnocoption as compared to patients performing strengthening exercises along. Thus proprioceptive exercises can be incorporated along with strengthening exercises in patients of knee ostooarthritia.
Conclusion
Management of ostecarthritis. which deleriorales with imbalance between the stress applied to the articular cartilage of the joint and its ability to withstand it, requires being more extensive than mere analgesics. This study between three groups comparing proprioceptive treatmant to strangthaning and strengthening and proprioceptive exercises suggest that combination of the two (proprioceptive exercises suggest that combination of the two (proprioceptive and strengthaning exercises) brings better relief to the subjects of knee ostoarthritis in reducing pain and functional disability. However, reposition error scores (joint position sense) did not improve sigificantly in proprioceptive and strengthening exercise group than other two groups. These results partly accept and parthy reject the experimental hypothesis suggesting that using proprioceptive exercises and strengthening exercises together will produce statistically significant difference in paln, disability and but joint position sense may take longer duration to show significant differenoes.
References
1. Lennart TH Jacobsson: Definitions of ostooarthritis in the knee and h a n d . A n n Rhaum Dis. 1996,55 (9) 656-8.
2. E M Badloy and A Tennant changing profile of joint disorders withage findings from a postal survey of the population of calderdale, WestYorkshire, United kingdom. Ann Rhaum Dis 1992 March: 51 (3) 356- 371
3. Fetson T.D. Zhang Y. osteoarthntis : New insight part l; The Diseaseand its risk factors. Ann. of inter Med 2000. 133 635-645
4. Leon Sokolott, some highlights in the emergence of modem concepts of osteoarthritis seminars in Arthritis and Rhaumatism volume 31,Issue 2, October 2001, Pages 71-107
5. Slemanda C. Heilman Dk: Reduced quadriceps strength relativeto body weight a risk factor for knee ostaoarthritis in woman? Arthritis Rheum1998 Nov 41 (11) : 1951-9
6. Charles slemenda. Dr. PH. Kenneth D. Brandt, ot al, Quadriceps Weakness and osteoarthritis of the knee, Ann intern Med 1997:127:97-104
7. Fischer N. M: Gresham G. E. Quantitative effects of physical therapy on muscular and functional performance in subjects with osteoarthritis of the knees Archlvas of physical medicine and rehabilitation 1993, vol 74,pp. 840-64
8. Ufuk Sekir and Hakan Gur Amulti-station proprioceptive exercise program in pationts with bilatoral knee osleoarthosis: functional capacity, pain and sensorimotor function. A Flandomized controlled Trial. Journal of sport science and Medicine (2005) 4, 590-603
9. David T. Felson, Md, MPH, K Douglas Gross, PT, ScD The effects of impaired joint position sense on the development and progression of pain and structural damage in knee osteoarthints Arthnts Rheum Author manuscript; available in pMC 2009 October 6.
10. Da-Hon Lin, Chien-Ho Janice Lin, Efficacy of 2 Non- we ight-Be aning int e rventions, proprioception Tralning versus strength Training, for patients with knee osteoarthnts A Randomized clinical Trial j Orthop s p o rts phys Ther 2009. 39 (6) 450-457
11. Gupts Abhishok Rajendra, joba chitra, khatrisubhash: A randomized controlled trial to study the effectiveness of proprioceptive exercises in osteoarthritis knee: The journal of Indian Association ofphysiotherapists 2007: Vol- 3:2: Oct 47-52
12. Gail D Daylo of al physical Thorapy Troatment Effectiveness for ostooarthritis of the knee : A Randomized comparison of supervised clinical Exercise and Manual Therapy procedures versus a HomeExercise program physical therapy vol 85, No. 12,2005, december, pp 1301-1317
13. Scott M. Lephart, Freddin H. FU. propriocaption and neuromuscular control in joint stability 2000. Pg 349-59
14. Fitzgerald GK. Childs JD. Ridge TM, Aglity and porturbation trainingfor a physically active individual with knee oslooarthritis. Phys Ther.2002 Apr. 82 (4) : 372-82.
15. Robert Topp, Woolley S. et al, The effect of dynamic vensus isometric resistance training on pain and functioning amongadulls with osteoarthritis of the knee Arch. Phys Med Rohab 2002 Volume 83. Issue 9, pages 1187-1195
16. Bollarmy N. Buchanan WW. Goldsmith CH, Camboll J. Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important pationt relevant outcomes to anti-rheumatic drug therapy in patients with osleoarthritis of the hip or knee. J Rheumatoy. 1988, Dec; 15 (12): 33-40
17. Ray Marks: peripheral articular mechanismsin pain production in osteoarthritis, Australian Journal of physiotherapy 1992, 38: 289-298.